Snoring is one of the most familiar sounds of the night. It drifts through hallways, settles into the quiet corners of homes, and becomes part of family stories. Although it may seem simple, snoring is a layered acoustic signature shaped by airflow, anatomy, and the shifting landscape of sleep. It is a sound created by the body’s nightly negotiation with gravity, muscle tone, and breath.
What begins as a familiar nighttime sound unfolds into a quiet story of how the airway behaves during sleep, how the body regulates temperature and muscle tone, how evolution shaped the human throat, and how culture interprets the noises that rise and fall in the dark. The aim is to explore these themes with scientific clarity and a sense of quiet wonder, offering a view of snoring that is both grounded in physiology and attentive to the subtleties of lived experience.
🌬️ What snoring really is: A sound born of air and tissue
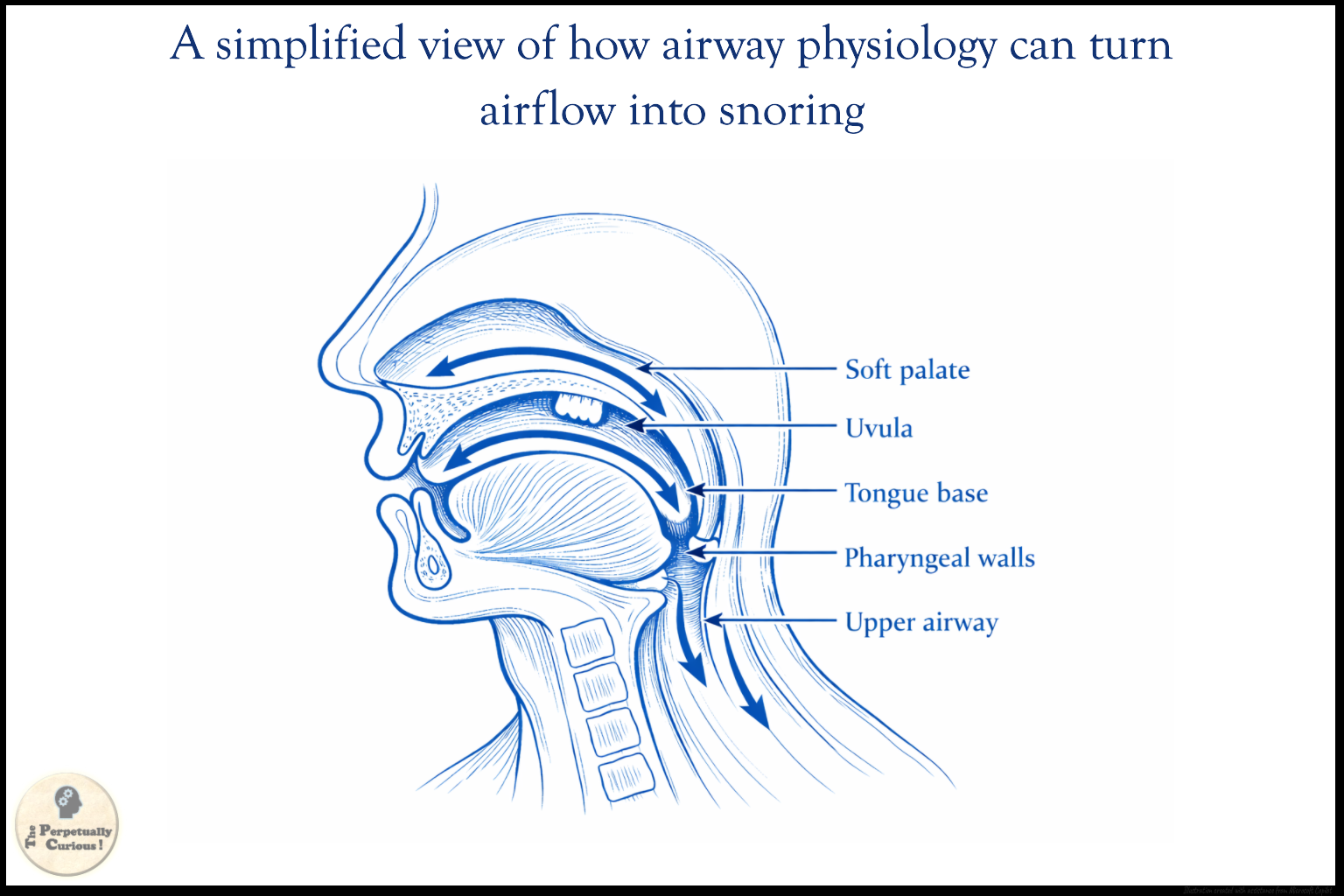
Snoring is produced when air flows through a partially narrowed upper airway during sleep and causes surrounding soft tissues to vibrate. The soft palate, uvula, tongue base, and pharyngeal walls are the most common contributors. When the airway narrows, airflow becomes more turbulent. This turbulence increases pressure fluctuations and sets the tissues into vibration, creating the sound recognized as snoring.
During sleep, muscle tone in the upper airway often decreases. As the muscles relax, the airway may become narrower than it is during wakefulness. The combination of reduced muscle tone, tissue compliance, and airflow volume creates conditions in which vibration becomes more likely. Snoring may be soft and intermittent or loud and continuous, depending on the degree of narrowing and the characteristics of the tissues involved.
That variation in sound begins, quite literally, in the architecture of the airway itself, where structure and physiology shape the pathways through which breath must travel.
🧠 Anatomy and physiology: The upper airway as a dynamic passage
The human upper airway is a flexible, muscular tube that must remain open to allow breathing while also supporting speech and swallowing. During wakefulness, a network of muscles maintains airway patency. During sleep, as the brain moves away from wakefulness and through the stages of non‑REM and REM sleep, neural drive to the upper‑airway muscles shifts, and this changing pattern of activation can make the airway more vulnerable to narrowing.
Several anatomical features may influence whether a person snores. A relatively large tongue, a low‑lying soft palate, or a smaller jaw may reduce the available space in the pharynx. In children, enlarged tonsils or adenoids may narrow the airway. In adults, increased soft tissue volume in the neck region may contribute to airway narrowing. Nasal airflow also plays a role, because nasal resistance may alter breathing patterns and encourage mouth breathing, which changes the dynamics of the upper airway.
Breathing during sleep is regulated by neural systems that respond to carbon dioxide, oxygen, and subtle shifts in respiratory effort. These systems adjust the timing and strength of muscle activation in the upper airway, coordinating airflow with the body’s chemical signals. This interplay reflects the broader importance of neural communication, where breathing, airway tone, and sleep state are shaped by changing signals rather than fixed mechanical parts.
These anatomical and physiological features do not remain constant throughout life. Their evolution across childhood, adulthood, and older age influences how snoring appears at different stages.
👶 Snoring across the life course: From childhood to older adulthood
Snoring occurs across all age groups, but its causes and implications may differ with developmental stage. Habitual snoring, defined as snoring on most nights, has been reported in approximately 7 to 20 percent of children and about 20 to 50 percent of adults in various cohort studies. These ranges reflect differences in study design and demographic characteristics, yet they consistently show that snoring is common.
In children, snoring may be associated with enlarged tonsils and adenoids, which can narrow the nasopharyngeal airway. This pattern is most often observed during early childhood, approximately between 2 and 8 years of age, when lymphoid tissue can be proportionally large relative to the airway. In adolescents, increased body weight and craniofacial development may play a greater role.
In adults, snoring prevalence tends to increase with age. Muscle tone in the upper airway often decreases, and soft tissue distribution may change. Hormonal influences, craniofacial structure, and body composition may all contribute. As these life‑course changes accumulate, they may alter the stability of the airway during sleep, which brings the discussion naturally to the broader spectrum of sleep‑disordered breathing.
🩺 Snoring and sleep-disordered breathing: When sound meets syndrome
Sleep‑disordered breathing encompasses a spectrum of conditions in which breathing during sleep is altered. At one end lies primary snoring, where airflow is maintained and oxygen levels remain stable. At the other end lies obstructive sleep apnea, characterized by repeated episodes of partial or complete upper airway closure during sleep.
During obstructive respiratory events, airflow may be markedly reduced, as in hypopnea, or may cease entirely for defined intervals, as in apnea. These episodes may lead to drops in blood oxygen levels and brief arousals from sleep. Over time, recurrent events may be associated with cardiovascular, metabolic, and neurocognitive consequences. Snoring often appears before or after apnea events, creating a rhythmic pattern that reflects the airway’s struggle to remain open.
Chronic intermittent hypoxia, a hallmark of obstructive sleep apnea, involves repeated cycles of reduced oxygen followed by reoxygenation. These cycles can influence autonomic and inflammatory signaling, altering how the body regulates cardiovascular tone, stress responses, and metabolic pathways. Emerging research also examines how these physiological shifts may relate to the gut brain axis, which is increasingly recognized as a bidirectional network connecting neural, immune, and gastrointestinal processes.
Because snoring is both a sound and a physiological event, researchers have explored whether the acoustic properties of snoring can offer additional insight into airway behavior.
🎵 The acoustics of snoring: Loudness, frequency, and airflow signatures
Snoring is not a single sound but a collection of acoustic features. Researchers have examined loudness, pitch, and temporal patterns to understand whether they may provide clues about airway behavior. Loud snoring has been associated in some studies with a higher likelihood of sleep‑disordered breathing, particularly when combined with other indicators. However, loudness alone does not provide a definitive diagnosis.
The frequency content of snoring may reflect which tissues are vibrating and how airflow interacts with them. Vibration of the soft palate may produce different acoustic signatures compared with vibration of the tongue base or lateral pharyngeal walls. Some studies have explored whether specific frequency bands correlate with particular anatomical sites of narrowing.
Temporal patterns also matter. Snoring that occurs in clusters, coincides with pauses in breathing, or changes with body position may carry different implications from snoring that is stable and continuous. Researchers have used advanced signal processing techniques to analyze snoring recordings and to investigate whether acoustic markers can assist in characterizing sleep‑disordered breathing. Acoustic patterns can support this characterization, but they cannot diagnose sleep apnea by sound alone.
These acoustic patterns do not exist in isolation. They emerge within a broader web of anatomical, environmental, and social influences that shape how snoring appears in daily life. Listening to these patterns offers a way of hearing how the airway behaves during sleep, revealing subtle shifts in physiology that might otherwise remain unnoticed.
🌍 Risk factors, environment, and the human story around snoring
Snoring is shaped by anatomy, body weight, age, sex, and environmental exposures. Increased neck circumference, craniofacial structure, and nasal airflow patterns may all influence airway behavior. Environmental factors such as air quality, humidity, and allergens may also affect nasal airflow and airway stability.
Across populations, researchers have observed that sleep‑disordered breathing may vary with social and environmental conditions. Access to health care, occupational patterns, and exposure to pollutants may all play roles. These factors intersect with biological predispositions to shape how snoring appears in different communities.
Beyond these biological and environmental influences, snoring also carries a social and cultural dimension that varies widely across settings. It may influence sleep arrangements, become part of family narratives, or be interpreted differently across cultures. Some cultures treat snoring with humor, while others view it with concern. These interpretations highlight the human context in which snoring occurs.
Beyond these influences lies the deeper mystery of sleep itself, where snoring becomes one of the many subtle expressions of the body’s sleeping rhythms.
🌙 Snoring as a window into sleep: The quiet complexity beneath a familiar sound
Sleep is an active state in which the body shifts through stages that each create a different airway landscape. Light sleep may preserve more muscle tone. Non‑REM sleep brings progressive relaxation with each deeper stage, while REM sleep introduces a paradox of vivid dreaming and near‑complete muscle atonia, creating the most permissive conditions for airway narrowing.
These shifting stages reflect the body’s internal circadian and ultradian rhythms, which guide the nightly pattern of restoration.
Within this changing architecture, snoring appears as an audible trace of the body’s negotiation with gravity, anatomy, and breath. Some studies have observed that snoring may increase during slow‑wave sleep, even though the airway is less prone to complete collapse. This suggests that snoring reflects not only obstruction but also the changing neuromuscular conditions of sleep.
This nightly choreography also relates to the movement of cerebrospinal fluid, which flows through the brain in patterns shaped by slow waves in neural activity, blood oxygenation, and sleep depth.
By listening to snoring as part of the broader soundscape of sleep, one can appreciate how a seemingly simple noise arises from layered processes. It becomes a map of the night, marking the body’s journey through its internal landscapes.
Pass this article along to someone curious and let the learning travel.
💡 Did You Know
🌀 Some researchers have used computational airflow models to simulate how different airway shapes influence snoring patterns. These models help visualize how even small anatomical differences may alter airflow behavior.
🐒 Certain mammals, including some primates and domestic dogs, produce snoring‑like sounds during sleep. These observations offer comparative insights into how airway structure and neuromuscular control have evolved.
🏔️ Sleep‑related breathing may change at high altitude because lower oxygen availability can affect ventilatory control. These shifts more often reflect central breathing instability than ordinary snoring mechanics, although some individuals may notice changes in nighttime breathing patterns.
🌡️ Some researchers have proposed that the sleep‑related drop in core body temperature may indirectly influence airway muscle tone, although this relationship remains an area of ongoing study.
🔭 The human airway represents an evolutionary compromise between breathing and speech. The anatomical adaptations that support complex vocalization may also contribute to the airway’s vulnerability during sleep.
Is snoring always a sign of a serious condition?
Snoring is often a marker of increased upper airway resistance during sleep, but it is not always associated with a serious condition. In some individuals, snoring may occur without significant changes in airflow or oxygen levels.
Can snoring occur without apnea?
Yes. Snoring may occur without apnea when airflow remains adequate and oxygen levels remain stable. Snoring reflects increased airway resistance, while apnea involves partial or complete airflow reduction.
Do apnea events always produce snoring?
Not always. Some apnea events occur silently, especially when the airway collapses without preceding vibration.
Why does snoring vary from night to night?
Snoring may vary because airway tone, sleep position, nasal airflow, and environmental conditions can change from night to night.
Does nasal airflow influence snoring?
Nasal airflow may influence snoring because nasal resistance can alter breathing patterns. When nasal airflow is reduced, individuals may shift to mouth breathing, which changes the dynamics of the upper airway.
Is snoring influenced by seasonal changes?
Seasonal changes may influence snoring because humidity, allergens, and temperature can affect nasal airflow and airway behavior.
Why do some individuals snore only when they are very tired?
When individuals are very tired, muscle tone may decrease more rapidly during sleep onset. This reduction in tone may make the airway more vulnerable to narrowing and vibration.
Can altitude influence snoring?
Higher altitude can change sleep‑related breathing because lower oxygen availability affects ventilatory control. At altitude, these changes more often reflect central breathing instability than the obstructive mechanisms that produce snoring at sea level, but some individuals may still notice changes in snoring or breathing patterns when traveling to or living at higher elevations.
Can snoring sound alone diagnose sleep apnea?
No. Snoring acoustics may provide clues about airway behavior, but sound alone cannot diagnose sleep apnea. Diagnosis requires evaluation of airflow, oxygen levels, and sleep architecture.
Why can body position change snoring?
Body position can influence snoring because gravity affects how the tongue and soft palate rest within the airway. When lying on the back, these tissues may fall backward and narrow the airway more than in lateral positions.
In the stillness of night, the body traces its hidden pathways of breath and memory.
Each sound becomes a small reminder of how life moves through quiet spaces.
What rises in the dark is simply the body speaking in its oldest language.
💬 Sharing night stories, one breath at a time
If this exploration has offered you a new way of hearing a familiar night sound, sharing it can help more readers notice the quiet science woven into ordinary sleep.
Related articles
A wider collection of biological and health essays is available for readers who wish to delve deeper into the living processes, adaptations, and discoveries that shape life and well‑being.
If you would like to keep up with what unfolds here, the Updates page is the best place to begin.